Patient Inspection
Patient assessment is the key to diagnosing the patient properly. Effective inspection requires:
- Communicating with the patient
- Keeping patient privacy and confidentiality
- Monitoring cardiopulmonary signs and symptoms
- Assessing vital signs
- Performing a physical assessment
Communicating with the Patient
Nonverbal Communication
Nonverbal cues often tell you more than what a patient says out loud. Watch for:
- Body movement — guarding, restlessness, splinting the chest
- Facial expression — grimacing, pursed lips, flared nostrils
- Touch — pulling away, reaching for support
- Eye movement — tracking, avoiding gaze, darting eyes
Patient Privacy & Confidentiality
Provide the patient with the appropriate space for the moment of care. Edward T. Hall's proxemic zones give us a useful framework: as trust builds, you move closer — never the other way around.

Social Space
- Used by a therapist to help build and establish rapport
- Allows you to see the "big picture"
- 4 – 12 feet
Personal Space
- Used to garner sensitive patient information
- Allows the patient to be more comfortable sharing information
- 18 inches – 4 feet
Intimate Space
- Reserved primarily for physical examination and treatment
- To be done after establishing rapport and asking for permission
- 0 – 18 inches
Cardiopulmonary Signs & Symptoms
OLDCART — The Symptom Interview Framework
Whenever a patient reports a symptom, walk it through OLDCART:
| Letter | Stands For | What You're Asking |
|---|---|---|
| O | Onset | When did it start? |
| L | Location | Where is it? |
| D | Duration | How long does it last? |
| C | Characteristics | What does it feel like? |
| A | Associated manifestations | What else happens with it? |
| R | Relieving factors | What makes it better? |
| T | Treatment | What have you tried so far? |
Cough
A cough is a reflex triggered by stimulation of receptors in the pharynx, larynx, and large bronchi — most often from inflammation, mucus, or foreign materials. It is the most common symptom in patients with pulmonary disease.
Assessment Questions
- Dry or loose?
- Productive or non-productive?
- Acute or chronic?
- Does it occur more frequently at certain times (e.g., at night, with exercise, with cold air)?
Sputum Production
Sputum production is most often caused by mucous gland inflammation.
- Sputum — substance expelled from the tracheobronchial tree, pharynx, mouth, sinuses, and nose via coughing or throat clearing
- Phlegm — secretions from the lungs and tracheobronchial tree not contaminated by oral secretions
Color → What It Suggests
| Color / Appearance | Term | Commonly Associated With |
|---|---|---|
| Clear, colorless, egg white | Normal | Healthy lungs |
| White-gray, thick | Mucoid | Emphysema, pulmonary TB, early chronic bronchitis, asthma |
| Green / rusty / yellow | Purulent (contains pus) | Infection, pneumonia (H. influenzae, streptococci, staphylococci) |
| Yellow-green, mixed | Mucopurulent | Infection, cystic fibrosis |
| Brown | — | Smoker, old blood |
| Frothy pink | — | Pulmonary edema |
| Blood-streaked | Hemoptysis | Bronchogenic carcinoma, tuberculosis |
Consistency
- Thin
- Thick
- Viscous (gelatinous)
- Tenacious (extremely sticky)
- Frothy
Odor
Fetid — foul odor. Can indicate:
- Lung abscess — local collection of pus and dead tissue
- Aspiration — inhalation of foreign material into the lungs
- Anaerobic infection — bacteria thriving without O₂
- Bronchiectasis — repeated lung infections/inflammation that dilates the bronchi and bronchioles
Quantity
Scant · Small · Moderate · Large · Copious
Dyspnea (Shortness of Breath)
Dyspnea is the subjective experience of breathing discomfort — it consists of qualitatively distinct sensations that vary in intensity. It is difficulty breathing as perceived by the patient, and it can impair work, exercise, and activities of daily living (ADLs).
ADLs — Remember "DEATH"
- Dressing
- Eating
- Ambulating
- Transferring / Toileting
- Hygiene
Common Causes of Dyspnea
- Asthma (acute on chronic condition)
- Pneumothorax
- Pneumonia
- Pulmonary emboli
- Pulmonary edema
- Hyperventilation
- Poor physical conditioning
Dyspnea Assessment Scales
| Scale | Range | How It's Used |
|---|---|---|
| Modified Borg | 0 – 10 | Scoring with descriptive terms to rate dyspnea after a specific activity |
| American Thoracic Society (ATS) SOB Scale | 0 – 4 | Specific terms depicting degree of dyspnea; used with questionnaires to quantify dyspnea during ADLs |
| Dyspnea-12 Survey | 12 items | Quantifies breathlessness using 12 physical and psychosocial descriptors — used for asthma patients |
Pulmonary-Induced Chest Pain
Pulmonary-induced chest pain usually involves the chest wall or parietal pleura, and can be induced by pneumonia, lung abscess, and pulmonary infarction.
- Pleuritic pain (most common symptom) — sharp, stabbing pain normally felt during inspiration
- Chest wall pain — dull, constant ache
- Can also be caused by intercostal or pectoral muscles
Edema
Edema is soft tissue swelling resulting from abnormal fluid accumulation. It is associated with pulmonary, cardiac, kidney, and liver disease.

Peripheral (Dependent) Edema
When the right ventricle becomes enlarged and unable to pump all the blood to the lungs, the venous system engorges. Pressure pushes fluid out into the tissues.
- First seen in the lower areas of the body
- As heart failure worsens, edema accumulates in the abdominal organs and other extremities
Distribution Clues
| Pattern | What It Suggests |
|---|---|
| Bilateral | Pulmonary hypertension, heart failure, or venous insufficiency |
| Unilateral | Venous obstruction or deep vein thrombosis (DVT) |
| Pedal | Manifestation of chronic lung disease |
General Clinical Presentation
Pain Level
Everyone feels pain differently. Pain should be compared to the worst pain the patient has ever experienced in their life.
Questions to Consider
- What makes the pain better or worse?
- Is the pain gradual or sudden?
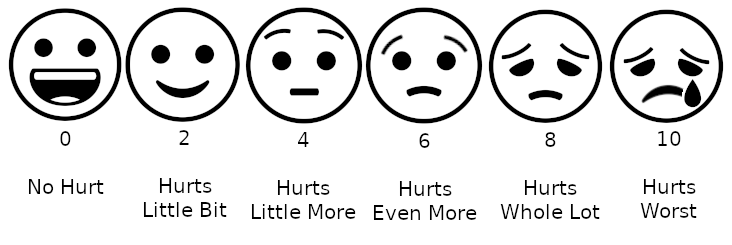
Wong-Baker Faces Scale
A 0 – 10 scale using facial expressions to grade pain — especially important for patients who can't communicate clearly (pediatrics, nonverbal, language barriers).
- 0 = smiling and pain free
- 10 = weeping in agony
Levels of Consciousness (LOC)
LOC exists on a spectrum. Become familiar with the language — you will chart these terms.
| Term | Patient Presentation |
|---|---|
| Sensorium | Baseline alertness and awareness |
| Confused | Disoriented but responsive |
| Delirious | Acutely confused, often agitated, hallucinations possible |
| Lethargic | Drowsy; arouses easily but drifts back |
| Obtunded | Difficult to arouse; responds slowly |
| Stuporous | Responds only to vigorous/painful stimuli |
| Comatose | No response to any stimuli |
Glasgow Coma Scale (GCS)
Observation begins the moment you first see the patient and continues throughout the exam. GCS is graded in three categories — total score ranges from 3 (deep coma) to 15 (fully alert).
| Category | Points |
|---|---|
| Eye opening response | 1 – 4 |
| Verbal response | 1 – 5 |
| Motor response | 1 – 6 |
Eye Opening Response (E)
| Score | Response | Description |
|---|---|---|
| E4 | Spontaneous | Eyes open and focused; patient recognizes you and follows eye movements |
| E3 | To speech / voice | Patient opens eyes when spoken to or directed to do so |
| E2 | To pain | Patient opens eyes only with painful stimuli |
| E1 | None | No eye opening |
Verbal Response (V)
| Score | Response | Description |
|---|---|---|
| V5 | Oriented | Can talk and answer questions about person, place, time — and the event that led to the current condition |
| V4 | Confused | Can talk and speak coherently, but not entirely oriented to person, place, time, and event |
| V3 | Inappropriate words | Answers with an inappropriate response, or excessive use of profanity not associated with anger |
| V2 | Incomprehensible words | Unintelligible words or sounds |
| V1 | None | No verbal response |
Motor Response (M)
| Score | Response | Description |
|---|---|---|
| M6 | Obeys commands | Patient follows simple motor commands |
| M5 | Localizes to pain | Reaches toward and attempts to remove painful stimulus |
| M4 | Withdraws from pain | Pulls away from painful stimulus |
| M3 | Flexion (decorticate) | Abnormal posturing; body curls into a protective posture by flexing the arms into the chest |
| M2 | Extension (decerebrate) | Body is abnormally extended; arms and legs may be extended and very rigid or difficult to move |
| M1 | None | No motor response |
Decorticate vs. Decerebrate — Visual Reference
Decorticate posturing (flexion toward the core — "de-cor-ticate" → arms to the core):

Decerebrate posturing (extension — a more ominous sign of deeper brain injury):

Clinical pearl: Decerebrate posturing generally indicates a worse prognosis than decorticate, because the lesion is deeper (midbrain/brainstem) rather than above the red nucleus.
Image Credits
- Personal Space — Edward T. Hall proxemic zones diagram, by WebHamster (CC BY-SA 3.0 / GFDL).
- Combinpedal.jpg — Pitting edema, by James Heilman, MD (CC BY-SA 3.0 / GFDL).
- Wong-Baker scale with emoji — emoji rendition of faces pain scale (CC BY-SA 4.0).
- Decorticate.PNG — by Delldot (public domain).
- Decerebrate.jpg — Wikimedia Commons (copyrighted free use).